|
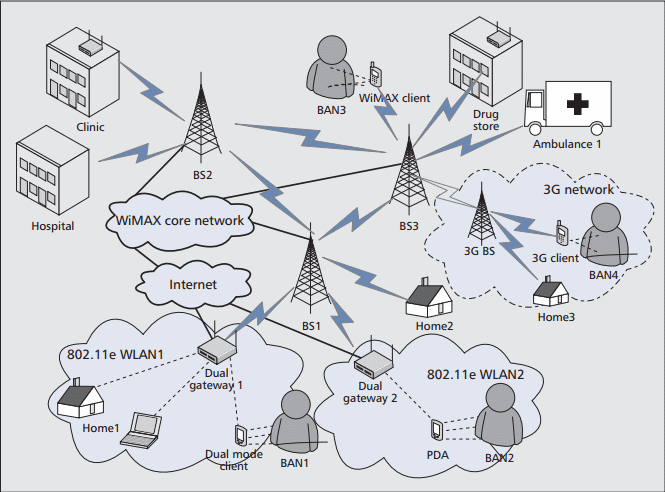
The integrated WiMAX and WLAN wireless telemedicine networks can be deployed in the following scenarios:
BANs: The BAN is a particularly appealing solution to provide information about the health status of a patient in medical environments such as hospitals or medical centers. The integrated 802.16/802.11 wireless-network-based tele-medicine system can also provide medical services for BANs through SM (BAN2 and BAN3) or DM (BAN1) mobile clients. The mobility of BAN2 is limited within WLAN2 due to only one WLAN interface being equipped with the client.
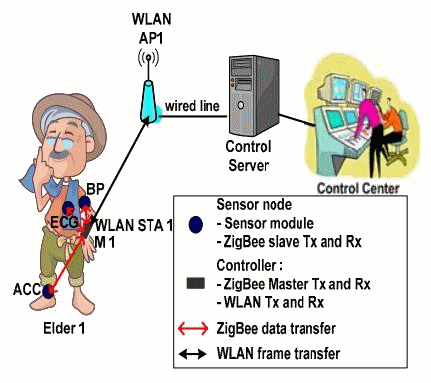
Figure below shows the health monitoring scenario for elderly people in a retirement community or nursing home.
The Electrocardiogram (ECG), Blood Pressure (BP), and 3-axis ACCeleration (ACC) signals located on the body of elderly people are monitored and recorded to the main control center (healthcare service provider).
There are two layers of network architecture in this system:
The first layer is defined by BAN, which constitutes the communication between sensors on the body with the controller on the wrist. The ECG, BP and ACC sensors measure and store medical signal in memory and data is sent to the controller periodically through the ZigBee technology. This is an uplink and unidirectional transfer. The ZigBee device in the sensor node operates as Slave (S) and ZigBee PAN Coordinator in the controller acts as Master (M). The controller receives data from all sensor nodes during the Contention-Free Period (CFP).
The second layer transmits the health care information received from ZigBee to the infrastructure network through WLAN. The controller acts as a 'gateway' that links BAN to the WLAN infrastructure. The buffered data in the controller is transmitted to the WLAN Access Point (AP) through IEEE 802.11b WLAN technology. This is also an uplink and unidirectional transfer. Fig below depicts the traffic pattern in a typical wearable health monitoring system.
For emergency cases, data transmission operates as follows.
When sensors detect a life-threatening sign, for example the ECG signal reaches a critical threshold, the controller shall recognize the danger, and transmits a warning message piggybacked onto the ECG data to the control center. An emergency team can be immediately dispatched to assist the elderly person in distress. Other WLAN traffics due to email or internet activities also exist in a health monitoring environment.
Home care network/Tele-Home Care: Home care is a growing field in healthcare and is a promising solution to the medical problems of modern society. The population census indicates an increasing trend of the senior population. Furthermore, modern life is becoming more stressful than ever; therefore, prolonged treatment is becoming more necessary. Home care via treatments in the patient's house with the assistance of the family reduces the need to transport patients between homes and hospitals.
In the integrated WiMAX and WLAN networks, patients may reside at home for remote patient monitoring through either connecting directly to a WiMAX BS equipped with a WiMAX client like Home2, or connecting to WLAN dual-mode APs like Home 1.
Intranet of a healthcare provider/intra-hospital services: WiMAX is a more practical and cost-effective solution for hospital intranet deployment due to the relatively larger coverage area of WiMAX networks than that of WLAN APs. The deployment of a WiMAX network in a hospital will reduce operation and maintenance costs, while offering full mobility support for patients and medical staff.
Clinics and drugstores: In contrast to a hospital, WLAN APs can likely provide enough coverage for clinics and drugstores. Therefore, dual mode WLAN APs can be deployed at clinics and drugstores to communicate with healthcare centers through WiMAX interfaces and to provide local wireless coverage through WLAN inter-faces.
Wireless video telephony: A number of telemedicine applications are based on the transmission of medical video, such as remote medical action systems, patient remote tele-monitoring facilities and transmission of medical videos for educational purposes. High quality videos/images are required to ensure proper diagnosis and/or assessment. Video transmissions over a WiMAX network have proved to be an effective and efficient platform in providing proper video content delivery.
VoIP services: WiMAX can also be used for VoIP services. Telephone bills can be drastically reduced as a result of the use of VoIP for communications among hospitals.
Quality of Service Support for Telemedicine:
QoS support is vital in integrated WiMAX and WLAN for e-healthcare service because various types of time-sensitive data should be communicated in such a service. For example, real-time communications and large enough bandwidth is required for transmitting high-resolution digital videos and images in mobile robotic systems. Providing QoS in the integrated IEEE 802.16/WiMAX and IEEE 802.11/WLAN network is a challenging issue. The need for efficient
interworking between IEEE 802.16/WiMAX and IEEE 802.11/WLAN arises in order to support QoS for delay-sensitive and bandwidth-intensive applications.
IEEE 802.11e employs a channel access function, hybrid coordination function (HCF), to support QoS provisioning in IEEE
802.11/WLAN networks. HCF uses both a contention-based channel access method, enhanced distributed channel access (EDCA), for contention-based transfer, and a controlled channel access, referred to as HCF controlled channel access (HCCA), for contention- free transfer. EDCA and HCCA provide QoS support over existing distributed coordination function and point coordination function schemes, respectively. EDCA defines four access categories (ACs): AC_VO with highest priority, AC_VI, AC_BE, and AC_BK with lowest priority corresponding to voice, video, best effort, and background traffic, respectively. The priorities are achieved by differentiating the contention window (CW) size and arbitration inter frame space (AIFS) time. Therefore, higher-priority ACs have smaller CWs and shorter AIFSs. The EDCA mechanism can only provide relative differentiation among service categories, but not absolute guarantees on throughput and delay performance, and it may thus starve lower-priority flows. HCCA provides QoS service by using signaling, scheduling and admission control. It defines a super frame containing a contention-free period followed by a contention period. During the contention-free period, only nodes which are polled by the AP are eligible to transmit for a burst period assigned by the AP. IEEE 802.11e defines eight traffic categories (TCs): TC6 and TC7 for voice, TC4 and TC5 for video, TC0 and TC3 for best effort, as well as TC1 and TC2 for background information. When a new TC starts, the node needs to send a service request to the AP providing its traffic specifications so that the AP will perform admission control to decide whether to allow the new flow for service.
In the delivery of medical data, some type of data such as real-time medical video streaming requires strict QoS support. In order to support such requirements, the extension of the standard 802.11e EDCF scheme, referred to as medical channel-adaptive fair allocation, has been proposed [13].
Different from IEEE 802.11/WLAN, IEEE 802.16/WiMAX was designed from the beginning with QoS in mind and defines five different types of services for different types of traffic flows as follows:
-
Unsolicited grant service (UGS) supports constant bit rate traffic, such as voice over IP (VoIP).
-
Real-time polling service (rtPS) supports real-time service flows which generate variable size data packets on a periodic basis (e.g., MPEG video). This scheme can guarantee QoS service to meet delay requirements.
-
Extended real-time polling service (ertPS) is a new scheduling algorithm for VoIP services with variable data rates and silence suppression.
-
Non-real-time polling service (nrtPS) is designed to support non real-time service flows that require variable size data grant burst types on a regular basis, such as high bandwidth FTP.
-
Best effort (BE) supports services that do not provide QoS guarantees (e.g., Web and email traffic).
|